 While attending the recent Healthcare Systems Process Improvement conference in New Orleans, I had the opportunity to attend a symposium that explored simulation modeling and its role in healthcare process improvement.I was astounded by the depth of the work being done by industrial engineers and simulation consultants for healthcare organizations. One prominent health system, known for its innovation, shared their work addressing the complex network of delivered items to their inpatient units. This included medications, linen, supplies, equipment, mail, food etc. Through a detailed study and subsequent simulation model they tested several distribution scenarios and were able to develop a plan that resulted in a savings of $3 million in nursing hours a year and required no change in the physical environment. Most inspiring was how the organization utilized these savings; rather than reduce staff, these hours were reinvested in direct patient care. $3 million worth of nursing hours now goes back to patients. This is an example of innovation driving quality.
While attending the recent Healthcare Systems Process Improvement conference in New Orleans, I had the opportunity to attend a symposium that explored simulation modeling and its role in healthcare process improvement.I was astounded by the depth of the work being done by industrial engineers and simulation consultants for healthcare organizations. One prominent health system, known for its innovation, shared their work addressing the complex network of delivered items to their inpatient units. This included medications, linen, supplies, equipment, mail, food etc. Through a detailed study and subsequent simulation model they tested several distribution scenarios and were able to develop a plan that resulted in a savings of $3 million in nursing hours a year and required no change in the physical environment. Most inspiring was how the organization utilized these savings; rather than reduce staff, these hours were reinvested in direct patient care. $3 million worth of nursing hours now goes back to patients. This is an example of innovation driving quality.
Similarly, a large community hospital explained their use of simulation to identify and quantify the potential risk of severe Operating Room (OR) disruption due to observation patients remaining in the recovery area overnight. Before a new building opened, they were able to determine the impact of these patients and develop an alternate strategy to avoid the loss of surgical capacity and the resulting revenue. This is real evidence-informed practice. Unfortunately, this was an example of a post-design simulation used long after it might have influenced the physical configuration or assumptions about the needed number of recovery positions.
A spirited debate broke out; why was a new building operationally deficient before it opened? Someone said benchmarks. It’s easy to see how this might have happened. The number of recovery positions was likely determined using benchmark ratios based on the planned number of procedures and ORs. But those benchmarks don’t account for overnight patients or the variation and disruption they would cause from early morning to mid-day. It won’t be constant or linear and so a static ratio is insufficient to determine room need without the risk of overbuilding.
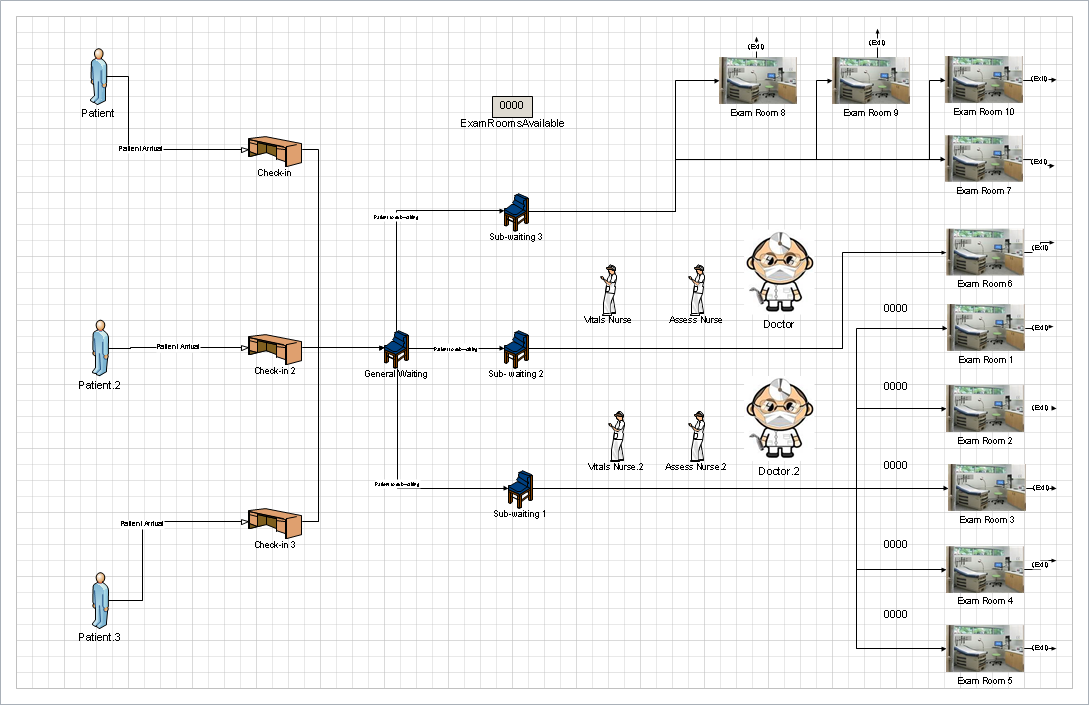
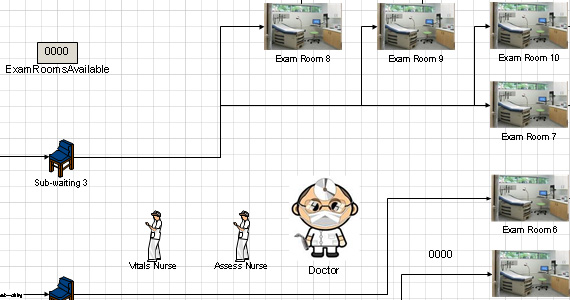
At Array, we have been developing simulation modeling capability to address this very situation. As we work with our clients to develop new facilities and improved processes, we need to understand the impact of their specific realities rather than national averages. As healthcare providers look to spend their precious capital dollars wisely, we can use simulation modeling to ensure their resources are devoted to adding value and improving care. To further aid this work, we also use ‘real-time tracking devices’ so that we can work with clients to gather actual current condition data from their organization. This data allows us to then build a more powerful simulation model, which becomes the foundation for testing new solutions long before the design is complete.
I am inspired by the great work being done to improve the quality of care and the stewardship of resources within our industry. These tools allow us to work with our clients to develop new solutions with a confidence that previously couldn’t be achieved until a post-occupancy evaluation. The benchmark may no longer be the best tool for designers. Simulation modeling can provide true data for a specific organization with specific needs. That is powerful knowledge when deciding what to build.



